a) Drying the canals with paper points:
This is yet another step which is very underestimated and skipped by many practitioners. Drying the canals is mandatory to achieve good bonding of obturating material and canals.
b) Common obturation techniques:
There are various obturation techniques and using any one of them would be fine. Honestly speaking, if the canals are cleaned well and dried properly, the technique of obturation does not have much impact on the success and failure of tooth.
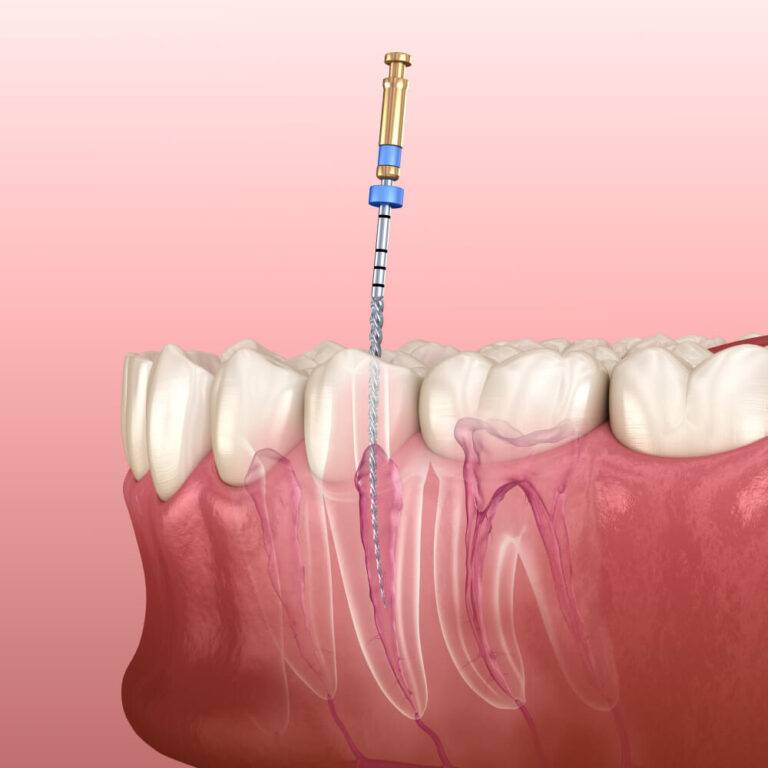
I. Single cone technique:
This technique works fine for molars and upper premolars. Make sure the single cone fits tightly in the canal, especially at the apical third and is well coated with sealer.
Palatal canal in maxillary molars and distal canal in mandibular molars have to be cross checked and if needed lateral gutta percha cones should be compacted.
II. Lateral compaction technique:
Ideal technique for anterior teeth and lower premolars with single canals. Try to achieve three dimensional obturation with fluid tight seal (no lateral spaces).
III. Down pack and back fill technique:
Another great and easy technique which can be used in all teeth. However, it requires specific obturating armamentarium which is not available in all dental set ups.
c) Sealing the gutta percha:
It is very important to seal the gutta percha exactly at the orifice of canals. Make sure there is no remanant gutta percha in the coronal cavity as it may affect the placement of permanent restoration.
It is best to seal one canal at a time and not altogether.
d) Cleaning the cavity after irrigation:
Clean the cavity with either saline or isopropyl alcohol and dry it properly with cotton pellet. Any contamination in the cavity with affect the permanent restoration.
e) Sealer puff:
Not desirable. Neither harmful.
It may cause temporary post-operative pain which can be controlled by medications. It is important to understand the difference between sealer puff, sealer extrusion and over filling.
f) Under and over obturation:
As long as the bio mechanical preparation is done properly and the canals are clean and sterile, a little short or a little over obturation is fine and wont effect the outcome of the treatment.
Anything in excess is not acceptable and if it happens then the obturation should be repeated.